
"Just before I went into the operating theatre, Dr Maguire said: 'How do you feel about having a robot do your surgery?'" says Catherine Butler. "I thought, 'I don't care if the cat does it as long as you get it out of me'," She laughs. "But I just smiled and said, 'yeah okay'. Then they wheeled me into the theatre and this big machine was there and I thought, 'that must be him'."
What Catherine, a recently retired medical receptionist, wanted “him” to get out of her, was a tumour on her kidney, though the robot that performed Catherine’s surgery isn’t quite a “him”. In fact, it’s got a female American accent which it deploys to self narrate as it performs certain manoeuvres. “Targeting complete!” it intones flatly at one point or “Docking arm!” it says at another.
“Da Vinci” is printed on the side of the robot, but this is just the name of the model and, disappointingly, not its actual name.
Have they named it? “I just call it ‘mine’,” says Barry Maguire and he laughs. “My robot.”
Does it have a personality? “It depends on the surgeon,” says Maguire. “Sometimes it has a big ego.”

Maguire is a urologist at St Vincent's University Hospital who spent three years in the Chicago being trained in how to use the technology. The kidney surgery I've come to watch (not on fully-healed Catherine, she is home and recovered) is overseen by Maguire and fellow urologist David Mulvin, who 20 years ago pioneered urological keyhole surgery in Ireland, albeit not of the remote-controlled robotic variety.
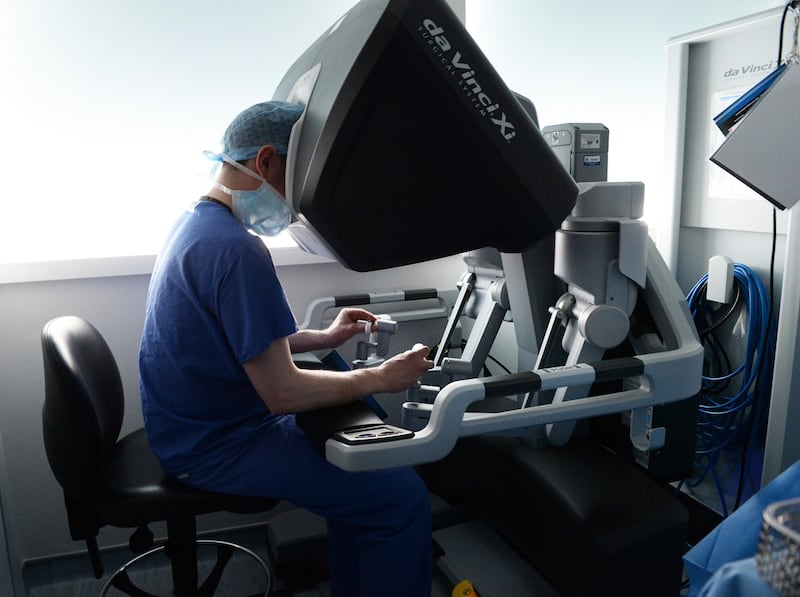
The robot is big and white and accompanied by a full surgical team of nurses and anaesthesiologists. It moves around on small wheels and it has four large mechanical arms that are operated by Maguire, who sits at a console in the corner, his head in a sort of groove where he can watch a detailed camera feed from inside the patient, and his hands rest on responsive controls and pads.
Monopoly
There are now several such robots in hospitals around Ireland though this is one of the few currently found in a public hospital. All are made by a US company called Intuitive Surgical which has a bit of a monopoly on the surgical robot business.
"They cost around two million," says Maguire, "and it costs well over €100,000 a year just for a service contract. The disposable equipment is very expensive. The public purse has not been interested in entertaining that so far. Our robot was given to us through Des Winter, one of the surgeons here, who has connections with big philanthropists. The Irish system is currently getting their robots through generous donations [via the St Vincent's Foundation]."
In St Vincent’s, much of this robotic surgery is done on kidneys and prostates. “In America over 90 per cent of people who have prostate surgery have it done robotically and the 10 per cent that remains are older surgeons,” says Maguire. “We’re just lagging behind because we physically don’t have the robots. It’s just about money . . . Ideally, you like to see a robot in each major high-volume hospital in Ireland.”
“The American hospitals have 10 or 12 robots,” says David Mulvin. “The private operators there realised very quickly that this was the way to go for certain operations because they can charge the same, but the reduced bed stay time was a huge thing for them.”
This touches on something that is of significant interest to the patients themselves. “There’s much less pain with procedures like this,” says Maguire. “There’s much less scarring and a shorter recovery time . . . We’ve taken our lengths of stay for kidney and prostate cancer down by three or four days.” (Indeed, Catherine Butler tells me she was out of hospital within three day and was off on a holiday six weeks later).
“For us it’s a nicer procedure,” says Mulvin. “We can see the patient the next morning and they’re sitting up on the bed eating breakfast. There’s much less trauma.”

Before the operation Maguire shows me a 3D plaster print-out of the patient’s kidney and points out the lumpy tumour he will be extracting and notes the specific distribution of the veins and arteries. Each kidney is different, he says. Eighty per cent of tumours like this are found in scans for other things. In the past the whole kidney might be removed. Nowadays, thanks to keyhole surgery and robots, they can remove tiny tumours more easily and with a 95 per cent cure rate. “We never give you the 100 per cent in medicine,” he says.
Tiny instruments
Maguire then shows me the tiny instruments, scalpels and scissors and clamps, that will soon be placed into the patient along with a camera via four small cuts in the patient’s side. “Then you sit at the console, which looks a bit like the Star Ship Enterprise, where your head is inside a machine that gives you this three dimensional high definition colour which is magnified,” he says. “It’s like wearing a large mask. Your arms are resting on a pad and your fingers go into these sensors that control the little arms you put into the patient… They work just like human hands. They rotate in the exact same manner as a hand.”
Does it have a distancing effect on the surgeon? He thinks not. “You lose your ability to touch and feel,” he says, “But the machine makes up for it in other ways.” He talks about how vivid and detailed the images are. “Sometimes it tricks you into thinking you can feel something.”
There is some resistance to robotic surgery among older surgical purists. Indeed, Maguire was at an event recently where a respected speaker scoffed at the idea of using robots. “There’d be the old school open surgeons who tut tut and say it’s not as good as touching and feeling. Their voices were very loud initially but they’re not so loud now.”
Younger surgeons are much more amenable to the idea, says Mulvin. “They’re used to using their iPhones and are very slick and learn how to use it very quickly.”
Soon I’m wearing scrubs and I’m in the operating theatre watching as the devices are introduced into incisions on a patient’s side. Maguire is in the corner at the console and the machine is beside the patient in the middle of the room, overseen by a scrub nurse and an anaesthesiologist. There are several other nurses nearby. Mulvin is standing beside me watching on a big screen the feed from the internal camera inside the patient’s body.
Soon tiny arms are cutting and moving the patient’s internal organs. “It’s a bit like defusing a bomb,” says Mulvin. “The kidney is tucked in under the liver . . . The bowel, the pancreas gland, the blood vessels, you’re peeling all these structures away.”
Chatting calmly
The operation takes over two hours with Mulvin and Maguire chatting calmly throughout and occasionally pointing out points of interest by electronically circling things on the screen (another feature of the technology). At one point, with the kidney now in sight, the blood vessels they’ve ascertained are likely to be pumping blood to the section of kidney with the tumour are clamped, and a timer is set for twenty minutes (if you restrict blood for longer than thirty minutes, says Mulvin, “it can lose function”).
And then I’m watching footage of a robot arm with a scalpel on the end cutting a cancerous tumour from a woman’s kidney. It is, as Mulvin points out to me, a different colour to the rest of the kidney and it sort of pops out eventually, like a tooth. Maguire then uses an electric current to seal the blood vessels and stop the bleeding (you can smell this in the room) before using the little robotic arms to sew up the wound. “He’s making it look quite easy,” says Mulvin with pride.
Maguire does all this from the console in the corner of the room without physically touching the patient. When this technology was originally developed it was envisioned that it would allow remote surgery on American soldiers in conflict zones. “The idea was that surgeons in America could operate while the robot’s arms were in the body of a soldier on the field,” says Maguire.
He doesn’t think remote surgery of that sort will ever be a norm because he doubts whether the necessary rapport with the surgical team would be possible in such circumstances. “And you’d really want to trust the wifi,” he adds. He does, however, believe that robotic surgery more generally will eventually account for the majority of operations in Irish hospitals.

“My head always wanders to what things will be like in 100 years,” he says. “Surgery could be dead. It may be seen as quite crude to physically chop something out when you have immunotherapy, whole body imaging or genetic manipulation… A hundred years ago we didn’t have anaesthetics, we didn’t have microbiology, we didn’t have penicillin, we didn’t have computers.”
He laughs. “And now we have robots doing operations.”










